Gotham Holistic - SMS Policy
- By booking a New Patient Appointment online, you give consent to receive appointment reminders by text. You may opt out by replying STOP. Frequency varies. Message and data rates may apply.
- We do not send marketing texts/sms.
- We will NEVER share your information with third parties for marketing purposes.
- In advance of a patient's first appointment, patients are required to review and sign the office policies document below, which specifies how and for what purpose we may send texts to deliver patient care. Patients always have the option to opt out of sms by:
- Replying STOP to any text message
- Emailing us at info@gothamholistic.com to update your preferences
- Call us at 646-255-1332 to update your preferences
Gotham Holistic - Office Policies
(Signature required for new patients in advance of attending first appointment)
Welcome to the Gotham Holistic – the Acupuncture office of Kristin Cheng, L.Ac., MSTOM. We want you to be comfortable and to receive the best care possible. Please do not hesitate to ask any questions you might have regarding your visit, your billing, or our policies.
Payment
We accept cash and credit cards for payment of services. All patients are required to place a card on file for enforcement of our cancellation policy and for resolution of outstanding balances. By signing below you consent to have your card on file charged for any outstanding balances.
Cancellation Policy
We ask that you please notify the office at least 24 hours in advance if you need to cancel or reschedule any appointment. All appointments canceled or rescheduled within 24 hours of the appointment will be subject to a fee equal to the full fee of the treatment scheduled, which will be automatically charged to your card on file. This fee also applies if you fail to show up for your appointment. Patients with a treatment package will have a session deducted from their package.
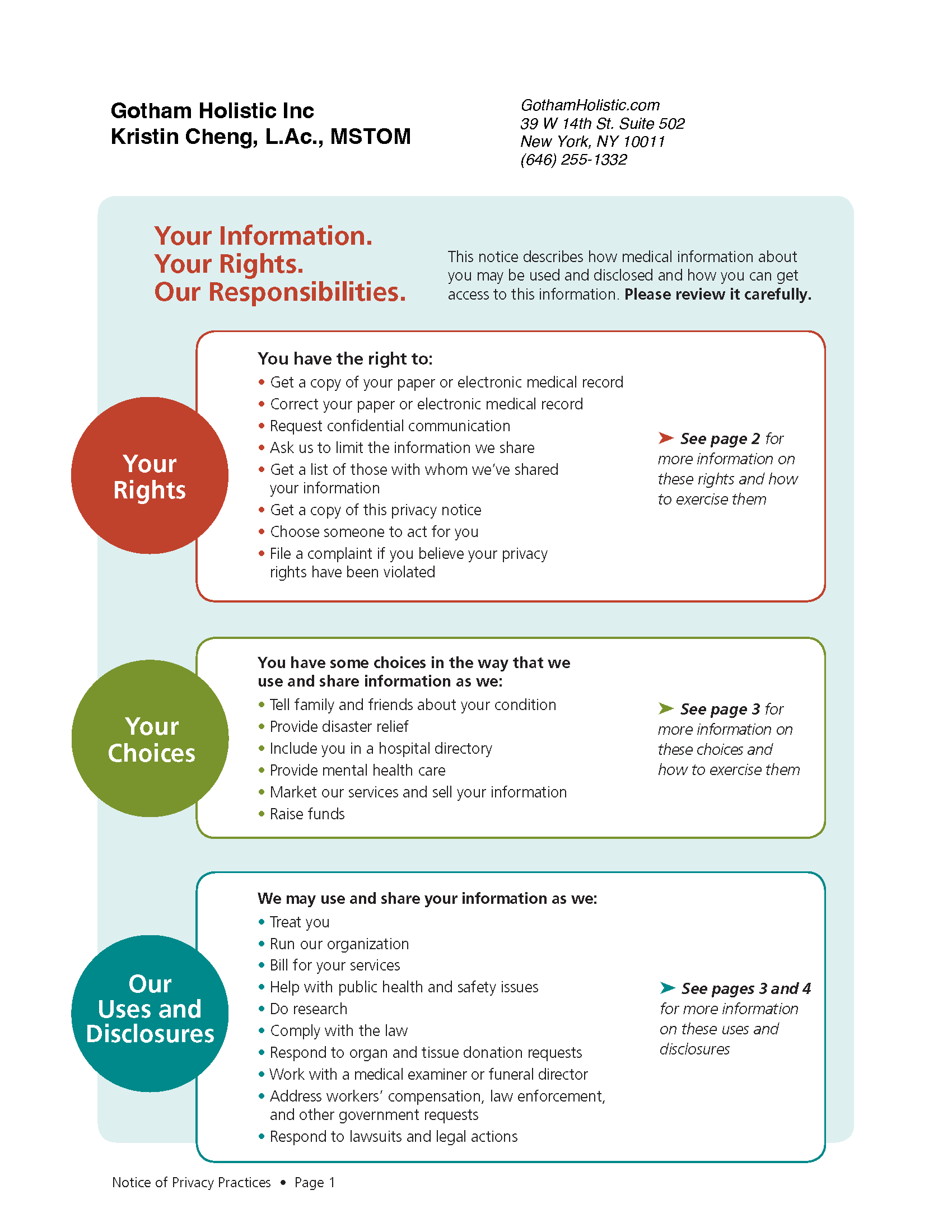
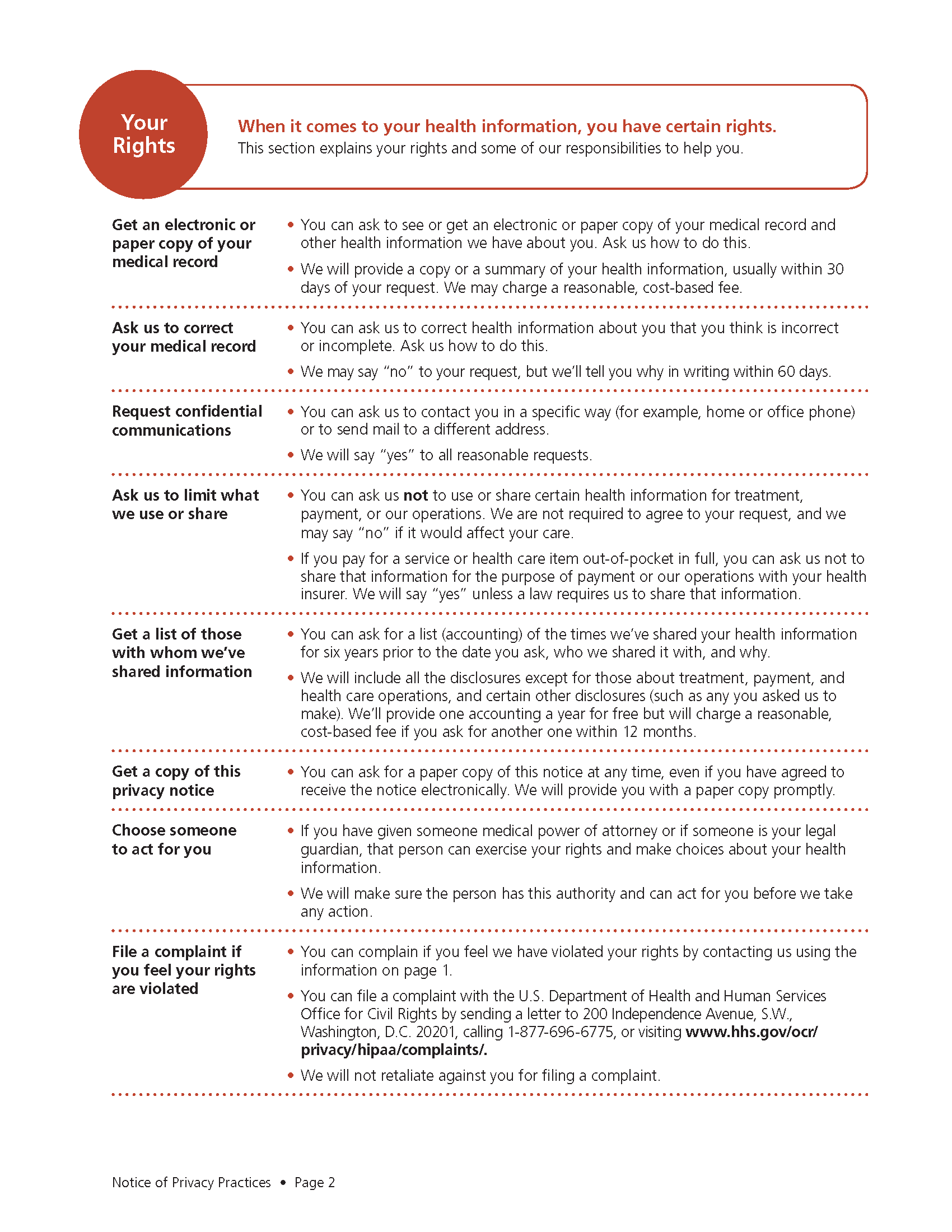
Patient Consent for Use and Disclosure of Protected Health Information
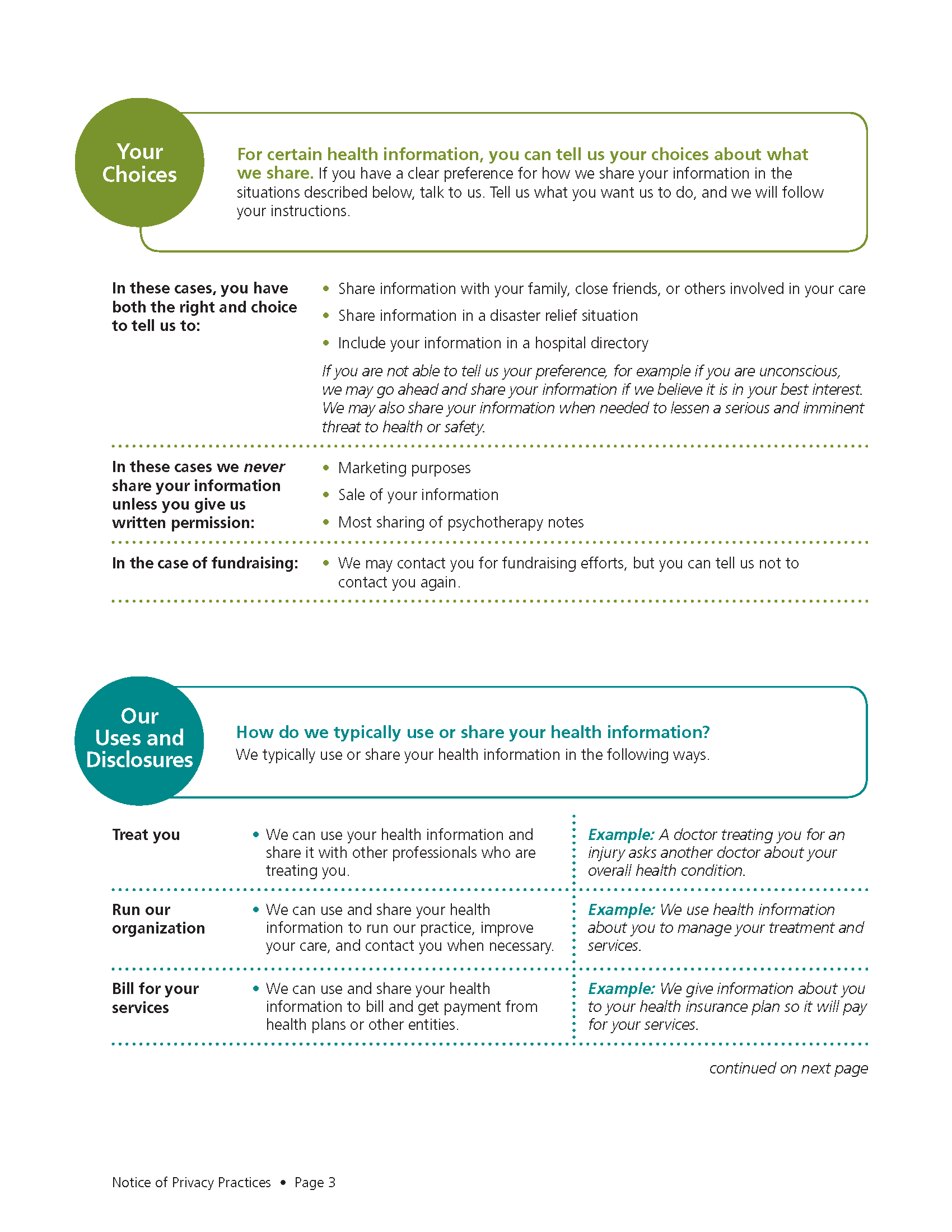
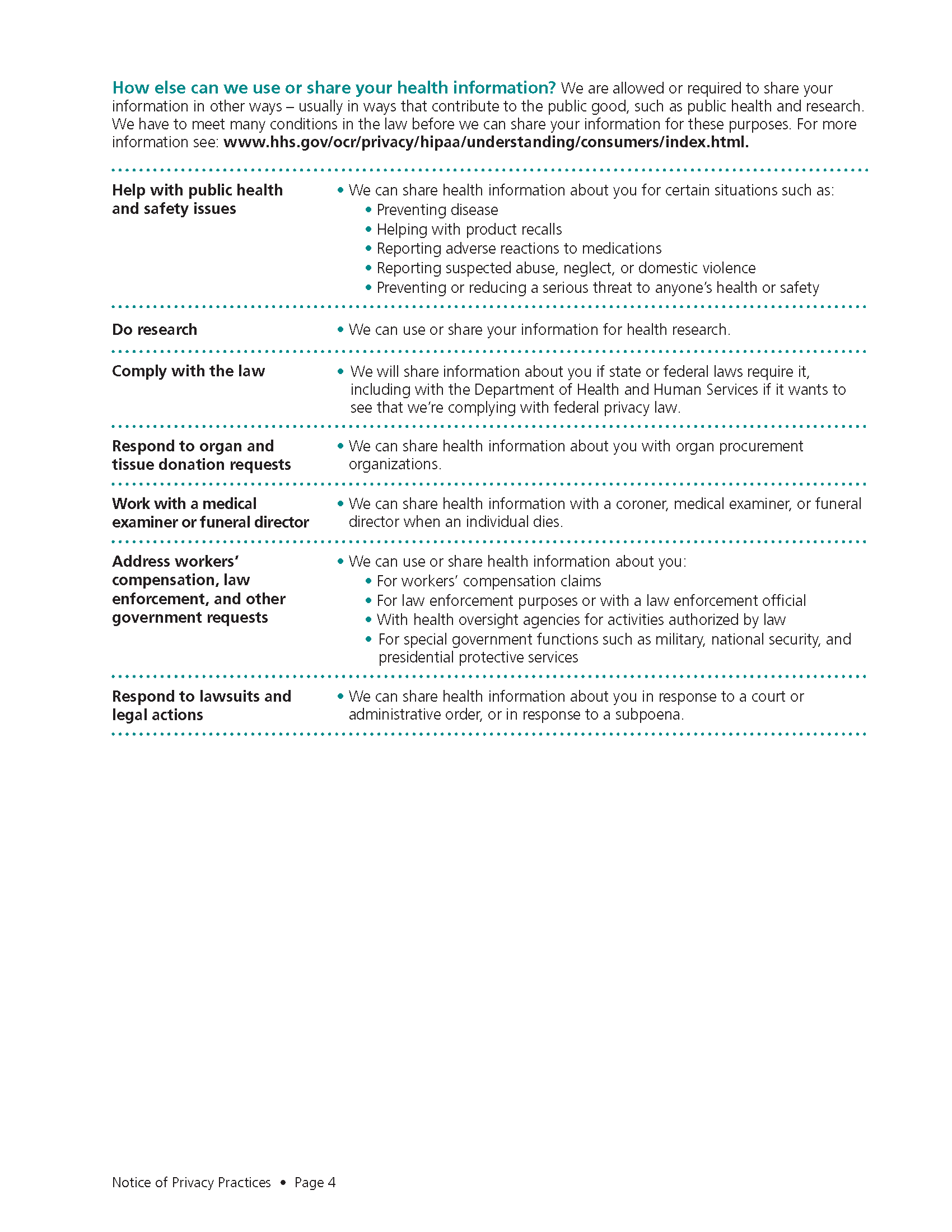
I hereby give my consent to Gotham Holistic Inc / Kristin Cheng, L.Ac. to use and disclose protected health information (PHI) about me to carry out treatment, payment and health care operations (TPO). (The Notice of Privacy Practices provided by Gotham Holistic Inc describes such uses and disclosures more completely.)
I have the right to review the Notice of Privacy Practices prior to signing this consent. Gotham Holistic Inc reserves the right to revise its Notice of Privacy Practices at any time. A revised Notice of Privacy Practices may be obtained by forwarding a written request to Gotham Holistic Inc, 39 W 14th St. Suite 502 New York, NY 10011.
With this consent, Gotham Holistic Inc may disclose all of my health information to other doctors/individuals involved in my care. This includes doctors/individuals that I have identified, as well as doctors/individuals which Gotham Holistic Inc may refer me to at any point in the future.
With this consent, Gotham Holistic Inc may call me at any phone number I have provided and leave a message on voice mail or in person in reference to any items that assist the practice in carrying out TPO, such as appointment reminders, billing and any calls pertaining to my clinical care.
SMS Policy:
With this consent, Gotham Holistic Inc may text me at my provided phone number(s) for general communication and in reference to any items that assist the practice in carrying out TPO, such as appointment reminders, billing and any texts pertaining to my clinical care. I understand that text messages are not encrypted or secure to the standards of HIPAA and HITECH. I understand that frequency varies and message and data rates may apply. I understand that I may opt out by replying STOP at any time. I understand that Gotham Holistic Inc will never share my information with third parties for marketing purposes.
With this consent, Gotham Holistic Inc may mail to my home or other alternative location any items that assist the practice in carrying out TPO, such as patient statements as long as they are marked “Personal and Confidential.”
With this consent, Gotham Holistic Inc may e-mail to any provided email address any items that assist the practice in carrying out TPO, such as general communication, appointment reminders, and patient statements. I have the right to request that Gotham Holistic restrict how it uses or discloses my PHI to carry out TPO. The practice is not required to agree to my requested restrictions, but if it does, it is bound by this agreement.
By signing this form, I am consenting to allow Gotham Holistic Inc to use and disclose my PHI to carry out TPO.
I may revoke my consent in writing except to the extent that the practice has already made disclosures in reliance upon my prior consent. If I do not sign this consent, or later revoke it, Gotham Holistic may decline to provide treatment to me.